Colon Cancer
Colon cancer is a type of cancer that occurs in the large intestine (colon) and sometimes in the rectum. It is often asymptomatic in its early stages and can be treated if caught early. Risk factors include a family history of colon cancer, being over 50 years old, and having certain digestive conditions.

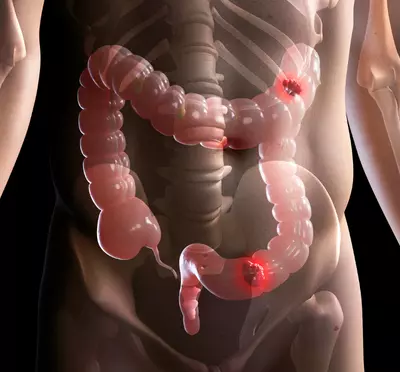
Overview of Colon Cancer
Colorectal cancer is a type of cancer that starts in the large intestine, which includes the colon and rectum. It can occur in any part of the large intestine and is more common than small intestinal cancer. Colorectal cancer develops gradually over a period of several years and can spread to other organs, such as the liver, lungs, and lymph nodes. It is recommended that people get a colonoscopy for colorectal cancer screening every 10 years after the age of 50. Colorectal cancer can be cured if detected early, and both men and women of any age can be at risk. It can be hereditary or occur spontaneously. In some cases, a person with a hereditary form of the disease may develop multiple primary cancers in different parts of the intestine at the same time.
Types of Colon/Colo-rectal Cancer
There are several types of colon and colorectal cancer, which are classified based on the type of cells in which the cancer originates. The most common type of colon cancer is adenocarcinoma, which starts in the glandular cells that line the inner surface of the colon and rectum. Other types of colon cancer include
Squamous cell carcinoma
This type of cancer starts in the thin, flat cells that line the colon and rectum.
Adenoid cystic carcinoma
This is a rare type of cancer that starts in the glandular cells of the colon and rectum.
Neuroendocrine tumors
These tumors start in cells that produce hormones in the colon and rectum.
Lymphoma
This type of cancer starts in the immune system cells of the colon and rectum.
Leiomyosarcoma
This is a rare type of cancer that starts in the glandular cells of the colon and rectum.
Carcinoid tumors
These are slow-growing tumors that start in the hormone-producing cells of the colon and rectum.
Sarcoma
This type of cancer starts in the connective tissue of the colon and rectum.
Causes of Colo-Rectal Cancer
Colon Cancer being one of the most common types of cancer, can be a serious and potentially life-threatening disease. Dr. Vasani has dedicated her career to understanding the causes of colorectal cancer and developing effective treatment approaches for her patients. Below are some known causes of colorectal cancer and how to reduce the risk of developing this disease, with a special focus on the insights and expertise of Dr. Sujata Vasani.
Age
Was a major risk factor a few years ago, with older age being the contributing factor. The cancer was commonly seen after the age of 50, and was an uncommon cancer in youth. Now however the trend is changing. A younger age is no longer a protective factor. More and more colon cancers are being seen in men and women below the age of 50, some being as young as 35 years. As such, all ages and both sexes are vulnerable.


Hereditary Colon Cancer
The majority of colon cancers seen below the age of 50 are hereditary. They are directly due to mutations inherited from either parent which result in the development of hereditary colon cancer syndromes like Lynch Syndrome (HNPCC) & Familial Adenomatous Polyposis (FAP).
Even in the absence of inherited mutations, a history of Colo-rectal cancer in a first-degree relative increases the risk of development of cancer in an individual.
An inflammatory bowel disorder
There are several factors that can increase a person’s risk of developing colon cancer. These include medical conditions such as Ulcerative Colitis and Crohn’s Disease, unhealthy behaviors like smoking and consuming alcohol, exposure to tobacco, a diet low in fiber, and a history of radiation treatment for cancer. People with Cystic Fibrosis, obesity, and diabetes also have an increased risk of colon cancer. Most cases of colon cancer in people over 60 years old are not inherited.
Colon/ Colo-rectal Cancer Pain

- Colon cancer often causes pain as it progresses.
- In the early stages, colon cancer may not have any symptoms.
- As the cancer develops, it can cause a loss of appetite, weight loss, and weakness.
- Abdominal pain may occur as the tumor grows and can be generalized or localized to the site of the tumor.
- The abdominal pain may increase in intensity as the cancer progresses and can be caused by blockage or perforation of the intestine.
- Invasion of nearby organs and lymph nodes can also cause severe abdominal pain.
Colon cancer in the rectum can cause progressively increasing pain at the site of the tumor. - Other symptoms of colon cancer include altered bowel habits, bleeding in the stool, and anemia.

Get screened for colorectal cancer and take control of your health today!
The mutations which are inherited from parents, and are passed on from generation to generation, are the causative factors for Colorectal cancer seen in younger individuals below the age of 50. These are risk factors that cannot be changed.
Hereditary Colon Cancer
Inherited colon cancer is a type of colon cancer that is caused by genetic mutations that are passed down from generation to generation. These mutations occur in specific genes and can result in the development of colon cancer at a young age, typically before age 50. Inherited colon cancer accounts for about 10% of all colon cancer cases and is more common in young adults. There are several different types of genetic mutations that can cause inherited colon cancer, including APC, BRCA, TP53, CHEK2, and MUTYH. The two most common inherited colon cancer syndromes are Lynch Syndrome (HNPCC) and Familial Adenomatosis Polyposis (FAP).
- Familial Adenomatous Polyposis (FAP)
Is a genetic syndrome that carries a very high risk of colon cancer, around 90% by the time a person reaches their mid-40s. It typically starts in the teenage years as multiple polyps throughout the colon and can progress to develop into cancer over 15 to 20 years. There is a slower-progressing variant called attenuated FAP that presents after age 50. FAP is caused by mutations in the APC gene.
- Lynch Syndrome or HNPCC
Lynch Syndrome is a genetic syndrome that increases the risk of colon and endometrial cancer, which often occur at a younger age. It is caused by mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, PMS2) and can result in multiple primary colon cancers and new primary cancers shortly after the initial tumor. These cancers are called Microsatellite High or Unstable (MSI) cancers and tend to respond well to treatment if diagnosed early.
10 early signs of Colon Cancer
Colon and Rectal cancer is usually asymptomatic in the initial stages. However, subtle signs and symptoms may develop which should raise an index of suspicion.
- Loss of appetite that may be gradual or sudden.
- Rapid weight loss, weakness, and fatigue due to appetite loss.
- Altered bowel habits or an alternating constipation and diarrhoea can occur as the presenting symptom of Colo-rectal cancer.
- Changes in bowel habits, including alternating constipation and diarrhoea.
- Blood in the stool, which may cause black stools and iron deficiency anaemia.
- Pain in the rectal area may be caused by a rectal tumour.
- Constipation that does not improve with medication, along with nausea, vomiting, and abdominal bloating may be caused by intestinal obstruction due to colon cancer.
- Pain in the back may be a symptom of colon cancer.
- Anemia may be caused by prolonged blood loss in the stool.
- Abdominal pain that may be localized or generalized.

Diagnosis of Colon / Rectal Cancer
In order to diagnose colon or rectal cancer, a colonoscopy may be conducted following bowel preparation to examine the entire bowel. If a mass is detected, a biopsy will be taken and sent for testing. A full body scan, such as a PET-CT or CT scan, may be conducted to determine the extent of cancer spread. In cases of a suspected rectal mass, a digital rectal examination or an endoscopic ultrasound or pelvic MRI may be done. Along with these tests, routine blood tests and a cardiac evaluation may also be conducted. A positive result on a stool occult blood test may also suggest a colon or rectal cancer diagnosis.
7 Colon Cancer Symptoms in Men
Change in bowel habits
such as diarrhea or constipation
Blood in the stool
which may be visible or detectable only through testing
Persistent abdominal pain
which may be a dull or sharp feeling
Narrow stools
which may be thinner than usual

Unexplained weight loss
which may occur even without changes in diet or exercise
Constant tiredness or fatigue
which may not be relieved by rest or sleep
A lump or mass in the abdomen
which may be felt during a physical examination.
Treatment of Colon/ Rectal Cancer
- Treatment of colon cancer : Stage 1 & Stage 2
In stage 1 colon cancer, there is no spread outside the intestine and chemotherapy is not usually necessary. Surgery alone is typically sufficient. In stage 2 colon cancer, surgery is usually enough if the cancer does not have any high-risk features, such as poorly differentiated or undifferentiated cancer, lymphovascular or perineural invasion, less than 12 lymph nodes examined during surgery, a high extent of tumour budding, presentation with intestinal obstruction or perforation, or invasion into surrounding tissues and organs (T4 primary). If any of these high-risk features are present, additional chemotherapy may be necessary following surgery.
All stage 2 colon cancer patients should have their tumour sample tested for mismatch repair deficiency (dMMR), which can be diagnosed through microsatellite instability (MSI) testing. Treatment decisions regarding chemotherapy after surgery are based on the dMMR/MSI status, with dMMR patients having a better prognosis.
- Stage 3 Rectal Cancer patients
Stage 3 colon cancer is a serious condition that requires aggressive treatment. The first step is typically surgery to remove the cancer and any affected lymph nodes. After surgery, chemotherapy is usually given to kill any remaining cancer cells that may have spread beyond the intestine. This chemotherapy can be given as a combination of pills and an injection, or through an IV. The chemotherapy regimen will depend on the specifics of the patient’s case, but options may include FOLFOX, Modified FOLFOX, or CapeOx. In some cases, radiation therapy may also be used, either before or after surgery. The specific treatment plan will depend on the extent of the cancer and the patient’s overall health.
- Stage 4 or Metastatic Colo-Rectal Cancer patients
Such patients have disease spread at the time of diagnosis, usually into the surrounding tissues, lymph nodes, liver and lungs. Virtually any organ in the body can be involved and extensive metastases may be already present at the time of diagnosis.
The liver is the organ commonly involved at the time of metastases.
In such patients, a curative or a radical surgery is not possible. These patients can achieve disease control with appropriate therapy but cannot be cured. The treatment intent is palliative with the aim being to improve and then maintain a good quality of life, relieve/avoid pain, halt disease spread & obtain control of the cancer. Surgery is only advocated if palliation is required, as in relieving intestinal obstruction due to the cancer, or to control bleeding from an ulcerated tumour. Other than this there is usually no indication for surgery.
All biopsy samples of the cancer must be sent for further molecular profiling and next generation sequencing. Mismatch Repair Deficiency and Microsatellite Status must be tested as well.
A dMMR status diagnosed by MSI-H ( microsatellite high) status opens up the option of using Immunotherapy upfront rather than chemotherapy. Such patients are usually younger and may have a Hereditary Colon Cancer Syndrome. They respond extremely well to Immunotherapy and can achieve excellent tumour control with prolonged disease survival.
In case of a proficient MMR status (MSS- microsatellite stable), Immunotherapy has limited benefit. Such patients must undergo detailed molecular testing to look for targetable mutations like HER2, NTRK and mutations that may reduce benefit from targeted therapy- like RAS, RAF. The entire panel of mutations must be tested. The results guide the therapy chosen.
Chemotherapy is required in MSS patients where immunotherapy is not an option. Regimens used are FOLFOX, CAPEOX, FOLFIRI & FOLFOXIRI. The protocol chosen depends on the patient profile like age, general condition, co-morbidities, previously treated or newly diagnosed. Usually a patient will be sequentially treated with all available drugs as the cancer relapses after periods of control.
RAS & RAF mutations usually reduce benefit from targeted therapies like Cetuximab & Panitumumab. In these patients a targeted agent like Bevacizumab is added to the chemotherapy protocol. This drug blocks the blood supply of the cancer and potentiates the effect of the chemotherapy.
Absence of RAS/RAF mutations allows the addition of Cetuximab or Panitumumab to the chemotherapy. Bevacizumab is also an option for these patients with chemotherapy.
HER2 or NTRK mutations require the addition of targeted agents directed towards these mutations.
Chemotherapy plus targeted therapy or Immunotherapy is recommended for disease control till there is disease control or development of toxicity. Discontinuing chemotherapy following cancer control and continuing only targeted therapy as maintenance is also a valid option.
Participation of young patients in promising clinical trials of new agents is recommended as available treatment options are exhausted.
Patient Case Studies
Case studies provide valuable insights into the treatment and management of individual cancer patients, informing oncologists’ decision-making and helping to improve care and outcomes for all patients. They also inform clinical guidelines and best practices, benefiting all cancer patients
Colon Cancer Risk factors you can not change
About Dr. Sujata Vasani
Dr. Sujata Vasani is a Hemato-Oncologist with 18+ years of experience in her field. She currently has her own clinic at Kemps Corner and is an Honorary Consultant at these renowned hospitals – Saifee, Breach Candy, Bhatia, Cumballa, and Dalvi.
Testimonials
Frequently Asked Questions
Colon cancer is a type of cancer that affects the large intestine (colon) and the rectum. It is also known as colorectal cancer.
Symptoms of colon cancer may include:
- A change in bowel habits characterized by alternating constipation and diarrhea
- Persistent abdominal discomfort.
- A feeling that your bowel does not empty completely
- Weakness or fatigue
- Unintended weight loss
The exact cause of colon cancer is unknown, but certain risk factors have been identified. These include:
- Aging
- A family history of colon cancer or colorectal polyps
- A personal history of colorectal polyps or inflammatory bowel disease (such as Crohn’s disease or ulcerative colitis)
- A diet high in red or processed meats and low in fruits, vegetables, and whole grains
- A sedentary lifestyle
- Smoking and heavy alcohol consumption
- Tobacco consumption
Colon cancer is typically diagnosed through a combination of tests, including:
- A physical exam and medical history
- A stool sample test to check for blood
- A colonoscopy, in which a doctor inserts a long, flexible tube with a camera into the rectum to examine the colon
- A sigmoidoscopy, which is similar to a colonoscopy but only examines the lower part of the colon
- A biopsy of any mass detected on colonoscopy
Treatment for colo-rectal cancer may include surgery to remove the cancerous tumor, chemotherapy to kill cancer cells, and/or radiation therapy to shrink the tumor. The type of treatment recommended will depend on the stage of the cancer and the individual patient’s overall health.
Stage 4 colon cancer cannot be cured, it can be controlled with chemotherapy and targeted therapy. The patient can remain pain-free and maintain his quality of life with treatment. Targeted therapy and immunotherapy are able to give patients longer survival than chemotherapy alone. The role of surgery is only for palliation and is only advocated to relieve symptoms like pain, bleeding and intestinal obstruction.
A port is a type of device used for continuous and long term intravenous chemotherapy. It is like a permanent intravenous line which can be kept for as long as required. It is best described as a tube or a cannula, inserted under anaesthesia, through one of the major neck veins. It is anchored beneath the collar-bone and is not visible from outside. Its circular end can be felt by the patient. It is not painful once inserted and does not restrict the patients activities or sleeping positions. It has a circular end, which is opened using a special needle when chemotherapy or any intravenous fluid is given, when the infusion is complete, the needle is removed and the port closes automatically. A port should only be opened by a trained Oncologist or chemotherapy nurse. There is no specific management needed from the patient’s side.
Yes, colorectal cancer hereditary genes can be passed on to children and grandchildren. The disease-causing mutations are transmitted from generation to generation.
The length of time it takes to cure colorectal cancer can vary depending on the stage of the cancer and the individual patient’s overall health.
No, the chemotherapy used in the treatment of colon cancer and rectal cancer does not cause any hair loss.
The risk of the colorectal cancer returning after treatment depends on the stage of the cancer at the time of diagnosis and the type of treatment taken. Stages 3 and 4 cancers have a higher risk of recurrence then stages 1 and 2. The tumour characteristics also determine the risk of recurrence.
Normal, home-cooked food, which is freshly cooked, and rich in vegetables must be taken during Colo-rectal cancer treatment. Raw food must be avoided to reduce the risk of infections. Liquid intake must be good, at least 3 to 4 litres daily, to maintain a good urine output. Fruits must be washed and peeled before eating. Dry fruits must be a part of the diet. if juices are taken they must be freshly squeezed.
Yes, chemotherapy is safe as long as it is administered under the close supervision of a Medical Oncologist. Close monitoring is required when it is being given. It must not be administered by doctors who are not qualified and trained for this procedure. Intravenous chemotherapy must be given in a hospital set up only.
A Leading Colon Cancer clinic in Mumbai
Take the first step towards better treatment by reaching out to our expert team at the Colon Cancer clinic in Mumbai. Schedule a consultation today!
